Peace for the World World ! Your War Our Lives

The Dalai Lama
A Brief Colonial History Of Ceylon(SriLanka)
Sri Lanka: One Island Two Nations
A Brief Colonial History Of Ceylon(SriLanka)
Sri Lanka: One Island Two Nations
(Full Story)
Back to 500BC.
Friday, January 22, 2016
Tackling The Burden Of Suicide In Sri Lanka

By Kasun Kodituwakku –January 21, 2016

Kasun Kodituwakku
Over 800,000 suicide deaths are reported every year, 75% of these
origination from the lower and middle-income countries predominantly
within Asia.
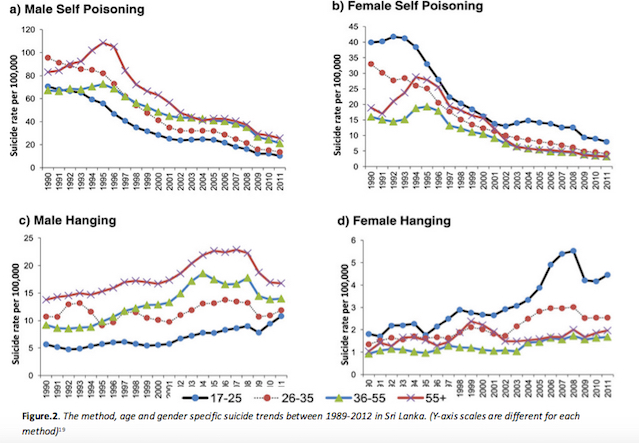
Sri Lanka was listed as having the 4th highest suicide rate
in the WHO report of 2014. The conflict-ridden history of the country
has meant that suicide has been a major burden of the previous three
decades, nevertheless the measures and interventions implemented by the
governing body has shown to positively impact suicide mortality rates,
particularly legislations on pesticides. But the numbers of attempted
suicides continue to increase, highlighting the inadequate attention
given to the central determinants of suicidal behaviour. Means
restriction and addressing social and economic factors whilst providing
mental support via a robust healthcare system have shown to be key in
tackling suicide.
 This
report explores the dynamics of suicidal behaviour in Sri Lanka and the
interplaying factors that contribute to the persistent national burden.
It investigates the education and employment systems as well as
assessing successfulness of interventions and policies implemented by
the governing body.
This
report explores the dynamics of suicidal behaviour in Sri Lanka and the
interplaying factors that contribute to the persistent national burden.
It investigates the education and employment systems as well as
assessing successfulness of interventions and policies implemented by
the governing body.
Burden of Suicide
Suicide is a complex multifaceted behaviour, which is induced by various
stresses and predispositions. It accounts for millions of non-fatal
hospital admissions and over 800,000 deaths annually, a life every 40
seconds.1 Projections estimate mortalities to almost double
to 1.53 million by 2025; with a further 15 to 30 million cases of
attempted suicide, thereby demonstrating the major global health burden
that suicide represents.2
Over 90% of suicides have been related to psychiatric illness in high-income countries (HIC)3, in which bipolar and major depressive disorders account for almost 60%.4
In the WHO 2014 report5, the overall suicide rate was
marginally higher in HIC than low and middle-income countries (LMIC),
12.7 per 100,000 and 11.2 per 100,000 respectively. But the sheer
population that reside in LMIC meant that it accounted for 75% of all
suicides.
Sri Lanka
Sri Lanka is a small densely populated island located just off the southeast shores of the Indian subcontinent6. It’s regarded as a lower-middle income country7 with a relatively low expenditure on health – $89 per capita 8, 3.4% of the GDP6,9.
But the widespread basic healthcare system available in Sri Lanka is
admirable considering its economic profile. An extensive network of
government funded public health units exists alongside a robust private
sector providing basic health care to the majority10.
Communicable diseases remain endemic in Sri Lanka; vector-borne diseases
like dengue fever along with diarrhoeal diseases and hepatitis A pose
the greatest threats6. Sri Lanka, like many LMIC, is facing
the double burden of disease, today non-communicable diseases account
for over 70% of mortalities, cardiovascular disease, chronic respiratory
diseases and diabetes are extremely prevalent10,11. Mental
health was previously a neglected topic, but in recent years especially
post-conflict (1983-2009) there has been a greater focus on such
conditions by the Ministry of Health. This resulted in the introduction
of mental health policies and interventions to tackle the health burden;
nevertheless only 1.6% of the total health budget is invested on mental
health12.